Shoulder Joint Replacement
Total Shoulder Arthroplasty
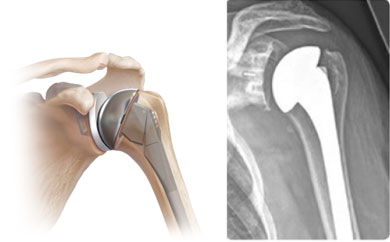
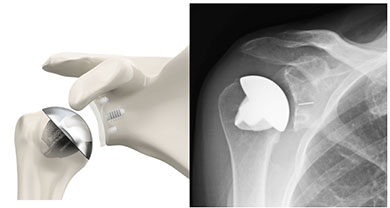
Total shoulder arthroplasty is a joint replacement surgery for a variety of painful shoulder joint conditions. The ball and socket portion of your shoulder will be replaced with metal and plastic parts that are similar in shape and size to your own shoulder anatomy. The socket portion of your shoulder is replaced with a plastic cup and the ball portion is replaced with a metal ball attached to a metal stem that is placed within the humerus. More recently surgeons are utilizing a less-invasive “stemless” humeral component.
Pictures of traditional shoulder replacement:
Pictures of stemless shoulder replacement:
Anatomy of the Shoulder:
The shoulder is made up of two joints, the acromioclavicular joint and the glenohumeral joint. The acromioclavicular joint is where the acromion, part of the shoulder blade (scapula) and the collar bone (clavicle) meet. The glenohumeral joint is where the ball (humeral head) and the socket (the glenoid) meet. The rotator cuff connects the humerus to the scapula and is made up of the tendons of four muscles, the supraspinatus, infraspinatus, teres minor and the subscapularis. The deltoid muscle is the muscle that forms the rounded curve of the shoulder. Tendons attach muscle to bone. Muscles in turn move bones by pulling on the tendons. The muscles of the rotator cuff keep the humerus tightly in the socket. The socket, or the glenoid, is shallow and flat. It is rimmed with soft tissue called the labrum that makes a deeper socket that molds to fit the humeral head. The joint capsule surrounds the shoulder joint. It is a fluid filled sac that lubricates the joint. It is made up of ligaments. Ligaments are soft tissue that holds bone to bone. Shoulder injuries can occur to any part of the shoulder.
Common Conditions that Require Total Shoulder Arthroplasty
Your surgeon may recommend total shoulder replacement for the following reasons:
- Osteoarthritis (degenerative joint disease)
- Rheumatoid arthritis
- Post-traumatic arthritis
- Avascular necrosis (osteonecrosis)
- A previous shoulder replacement that was not successful
- Failure of conservative treatments such as anti-inflammatories, cortisone injections, or physical therapy. Patients with a poorly functioning or torn rotator cuff, an axillary nerve injury, active shoulder infection or severe loss of bone stock on the socket or humerus are not candidates for shoulder replacement.
Expected Outcomes
Shoulder arthroplasty has been performed in the United States since the 1950’s. At that time it was used to treat severe shoulder fractures. In recent years it has become more common and is used for many painful shoulder conditions.
Most patients can be very active following a shoulder replacement. Golf, tennis, swimming and light yard work and gardening are allowed.
Preoperative Planning
Before your surgery it will be required to have preoperative testing. In some cases blood work, EKG (heart tracing), or a chest X-ray may be needed. If any of these tests are needed they will be scheduled for you and will be done during pre-testing when you meet with the anesthesia staff. If further testing is needed it will be arranged by the pretesting staff. If it has been some time since you have seen your primary care physician and you have a lot of medical problems, it would be best that you see your medical doctor before your pre-test date.
Your surgeon may also recommend advanced imaging studies such as an MRI or CT scan of the shoulder to assess the rotator cuff tendons and bone stock of the glenoid (socket) to determine if you are a candidate for a shoulder replacement and to help with surgical planning.
A recent study demonstrated decreased bacterial burden with the use of benzoyl peroxide scrub in the days leading up to surgery. It is therefore recommended that you scrub the operative extremity and armpit with 5% benzoyl peroxide gel for 3 mornings before surgery (the 3rd morning being the actual day of surgery). Apply the gel to the skin for 3 minutes prior to washing it away.
Your Surgery and Hospital Stay
You will arrive at the hospital approximately two hours before your scheduled surgery time. Procedures are performed on a “to follow” basis. Occasionally, a procedure scheduled ahead of yours may take longer than expected, so there may be some delay before your surgery. Regardless, it is important that you arrive on time. Sometimes an earlier procedure will cancel and we run ahead of schedule. You should not have anything to eat or drink after midnight the night before surgery. You may be advised to take some of your medications with a sip of water only. The anesthesia staff will discuss this with you at the time of your pre-testing. Upon arrival to the hospital you will go through a check-in process. At the appropriate time you will be brought into a pre-operative holding area. At this point the nurse will see you, review your records, and an IV will be started. A member of the anesthesia team will meet with you to discuss any anesthesia concerns and anesthetic options. Your surgery will be performed under general anesthesia (you will go to sleep.) In addition, the anesthesiologist may recommend a regional block if they think that you are a good candidate. This involves an injection of local anesthetic (numbing medicine) or placement of a catheter near the nerves at the base of the neck. These blocks are generally recommended to help control your pain following surgery. The anesthesiologist will discuss the risks of the block and the decision to perform this is a mutual decision between the patient and the anesthesiologist.
You can anticipate that your surgery will last approximately 2 hours, although this varies depending on the complexity of your surgery. If you have family members with you they will wait for you in the waiting room. Your doctor will speak with them after your surgical procedure to let them know that you are finished. During your surgery, family members should plan on remaining in or near the waiting area in order to be accessible at the completion of the procedure. Belongings will be stored in a locker in the pre-operative area. Please leave valuables at home or with family.
When you wake from surgery you will be located in the post-operative recovery room. Unfortunately family members cannot be present with you at this time as there are many other patients and many nurses in this area. Once you have been stabilized and are comfortable, approximately 1-3 hours after surgery, you will be transferred to the nursing division and you will be able to see your family. Most rooms on the orthopedic floor are private.
With advancements in technique and pain control, some patients go home the same day after surgery. Others will stay overnight or longer, depending on pain control or medical issues. If you are planning to go to an extended care or rehab facility you may need to stay 3 nights due to insurance reasons. If you are planning to go to one of these facilities you may want to research facilities in your area prior to surgery. The social work staff will assist with placement once you are in the hospital.
You will have a dressing on your shoulder and your arm will be immobilized in a sling. You may also have a drain in place to collect fluid and blood from the surgery. This will be monitored closely during your hospital stay. It will be removed the morning you are discharged. Other equipment you can expect to have while hospitalized includes: an IV until you are eating, drinking and voiding normally, a cold therapy unit in the place of ice bags, compression and sequential stockings on your legs to prevent blood clots, possibly oxygen tubing according to your needs, and possibly a catheter if you are not able to urinate normally.
As previously noted, you may be given a regional block. This block usually wears off sometime in the night. Your nurse will be offering you pain medication every 4 hours. We recommend that you begin taking the medication when it is offered so that you will have medication in your system when the block wears off. In addition to the routine pain medication you can ask for additional pain medication in IV or pill form if needed. Please ask for additional pain medication when you first begin feeling uncomfortable. You will also have medication for nausea if needed.
Lab work or “blood work” may be done during your stay. By looking at these results decisions are made regarding your care. In order for the lab results to be ready for your doctor in the morning the staff will collect samples from you. This is normally done between 12am and 2am. We apologize for any inconvenience this may cause you.
Occupational/Physical therapy will see you after your surgery to evaluate your needs, they normally start around 8am. You will begin doing range of motion exercises the morning after your surgery. The therapist will instruct you on these exercises. It is recommended to have a family member attend the therapy session if possible.
Risks and Complications
The list below includes some of the common possible side effects from this surgery. Fortunately complications are very rare in your doctor’s practice. Please note that this list includes some, but not all, of the possible side effects or complications. Complications may include complications from anesthesia, infection (very rare), nerve injury (extremely rare), blood vessel injury (extremely rare), bleeding (extremely rare), shoulder stiffness, failure of repair, failure to improve your symptoms as much as you had hoped, a stress fracture of the acromion bone where the deltoid originates (rare), a blood clot can form in your arms or legs and very rarely travel to your lungs, complex regional pain syndrome (a painful condition involving the arm, very rare).
Postoperative Care
- Sling instructions. After surgery your shoulder will be placed in a sling. The sling should be worn as directed by your doctor. You should wear your sling if you are up and about, or in large crowds, and while you are sleeping. You should remove the sling to shower, dress, and perform your range of motion exercises several times per day.
- We recommend that you eat a light diet the evening of surgery and the next day but you may resume eating a regular diet as soon as you tolerate it. Increasing fluids and dietary fiber (fruits, vegetables, and whole grains) in the weeks after surgery will assist with any constipation issues you may have from the pain medication.
- Pain control. When you are discharged from the hospital you will be given a prescription for pain medicine. You may take this medicine as prescribed. You will be discharged with your cold pack machine. This machine has a sleeve which is attached to an ice cooler. You place ice and some water in the cooler and plug this in to a regular outlet. This circulates cold water through the shoulder sleeve providing relief of pain and swelling after surgery. You should keep ice on the shoulder frequently for at least the first 48-72 hours after surgery. We urge icing 2-3 times per day for the first week especially before sleep. We do recommend that you put a t-shirt or a thin towel between you and the sleeve so that it doesn’t injure your skin.
- Wound care. If you are discharged with a clear dressing covering your incision you should leave it in place until your follow up visit with your surgeon. This type of dressing can get wet, so you may shower when you get home. If you are discharged with a white gauze dressing you may remove your dressing 5 days after surgery. After the dressing is removed you may then shower. You may not get in a hot tub or pool and immerse the incision underwater for four weeks but you may get in the shower and let the water run over them. Pat the incisions dry afterwards. There is no need to place any ointment over the incisions, it is better to keep them dry. Sometimes significant bruising is seen in the front of the shoulder or along the biceps muscle, forearm or even the chest/abdomen. This is normal and is related to mild internal bleeding after surgery. If you notice drainage from the incision, swelling or increased pain 5 days after surgery please call the office. Redness around the incision is very common and should not be a concern unless it is associated with drainage 5 days after surgery, redness spreading away from the incision or fevers.
- It is often very difficult to sleep following shoulder surgery. The surgery itself may interfere with your sleep-wake cycle. In addition, many patients have increased shoulder pain lying flat on their back. We recommend that you try sleeping in a recliner or in a reclined position in bed. This is often much more comfortable. You may place a pillow behind your elbow in order to move your arm away from your body slightly. You should wear your sling while you sleep, which may help with the discomfort of your arm moving. It can often take 2 months for sleep to normalize.
- Operating a motor vehicle may be difficult due to you inability to use your operative arm. If you should have an accident or get pulled over while wearing a sling, the authorities may consider that driving while impaired. Once you are out of your sling you may drive once you feel safe operating a vehicle. No one should operate a motor vehicle while taking narcotic medications.
- Physical therapy. In some cases you will begin your physical therapy/stretching exercises the morning after surgery. You will be instructed on these exercises by your surgeon and/or an occupational therapist. These exercises will be done 2-3 times per day while in the hospital and at home.
Medications to Avoid Before and After Surgery
Medications that increase the chances that you will bleed excessively after surgery include:
- Aspirin, enteric-coated, baby, and plain aspirin or any other product containing aspirin. In some cases, we may recommend stopping your aspirin 1 week before surgery. In others cases, low-dose aspirin may be continued based on your medical condition. Please discuss with your surgeon.
- Coumadin – discuss this with the prescriber as to the best time to stop this medication before surgery.
- Celebrex- stop 1 week prior to surgery.
- Ibuprofen (Advil, Motrin) - stop 1 week prior to surgery
- Naprosyn (Aleve) - stop 1 week prior to surgery
- Plavix – discuss this with the prescriber as to the best time to stop this medication before surgery
- Some over-the-counter herbs can also effect bleeding. These include chondroitin, dan shen, feverfew, garlic tablets, ginger tablets, ginkgo, ginseng, and quilinggao and fish oil.
After shoulder surgery, you should avoid continuous use of anti-inflammatory medications including ibuprofen (Advil, Motrin) and Naprosyn (Aleve) and any other prescription anti-inflammatories, unless your surgeon prescribes them. Do not resume these medications until your doctor says that it is okay. You may take Tylenol unless otherwise instructed not to do so.
Follow Up Appointment
PATIENTS ARE USUALLY SEEN IN THE OFFICE 7-10 DAYS AFTER SURGERY FOR WOUND AND RADIOGRAPHIC EVALUATION. IF YOU HAVE NOT BEEN SCHEDULED FOR A FOLLOW UP, PLEASE CALL THE OFFICE TO SET UP AN APPOINTMENT AT 310-665-7255. WE WILL THEN SCHEDULE YOUR SECOND FOLLOW UP APPOINTMENT FOR APPROXIMATELY 4 TO 5 WEEKS THEREAFTER.
Signs of an emergent situation include increasing redness, swelling, and significant drainage from the incision site, a fever greater than 101.5, inability to tolerate food and fluids after surgery. In rare cases, temporary breathing difficulties can occur in patients who have had a regional block or a pain catheter. If you find that you have any of these situations, it is advisable that you call 310-665-7200 anytime of the day or night when the office is closed so that emergent care can be initiated for you.
Please follow these instructions for emergency calls. During the business hours Monday to Friday, 8 a.m. to 4:30 p.m., except for Holidays, please call your surgeon’s nurse or medical assistant. For emergent calls during office hours, call 310-665-7200. The operator on call will contact your doctor’s staff.